
An evidence-based study reveals that dynamic standing in the Innowalk increases passive range of motion (PROM) and reduces spasticity in CP children, GMFCS IV and V. Statistically significant differences were found when compared to the effects of static standing.
The study, which included 20 non-ambulatory children with cerebral palsy (GMFCS IV-V), 5-17 years of age, shows the following:
- Passive range of motion increased in the hips in all directions after dynamic standing for 30 minutes and after 4 months of intervention.
- Spasticity in the hips decreased after 30 minutes of dynamic standing intervention.
Introduction
This newly published article breaks good news for non-ambulatory children with cerebral palsy. Children with gross motor function classified at level IV and V cannot walk or sit without support. Since they have severe functional limitations, and cannot independently move their joints through the full range of motion, they are at particularly high risk for developing contractures. Spasticity may also contribute to muscle shortening, torsional deformities, hip dislocation and/or scoliosis, which often causes pain and can affect motor control and function. In addition to increasing pain, these secondary complications of the CP-diagnose often lead to expensive treatments and hospitalization.
Among many different physical therapy interventions to prevent or reduce secondary complications, and to increase physical activity, standing intervention is one of them and recommended as standard care in most countries. There are two types of standing exercise training, static standing (StS) and dynamic standing (DyS). Static standing means that no lower body movement can be achieved while being in an upright position. Dynamic standing exercise is offered by the motorised medical device Innowalk. The device gives an opportunity to experience walking movements in an upright weight-bearing position.
There are few high-quality exercise intervention studies on children with CP, and the ones that exist have mainly been performed on ambulatory children with CP. A feasibility study done in Sweden, which included DyS in children with severe disability to advocate physical activity, showed that StS and DyS represent two different training modalities for non-ambulatory children. The outcome of this study encouraged the researchers at Lund University to study the effects of standing exercise training among severely disabled children further, and this is the first evidence-based research showing the effect on PROM and spasticity after standing exercise training among CP children GMFCS IV-V.
What is dynamic standing?
Dynamic standing allows people to experience reciprocal weight shift, flexion and extension of muscles and movement of the legs (and arms) in an upright weight-bearing position.
You find the full article “Non-ambulatory children with cerebral palsy: effects of four months of static and dynamic standing exercise on passive range of motion and spasticity in the hip” in the peer review journal PeerJ here.
To give you a brief overview of the study, here’s an article summary:
Aim of the study
Non-ambulatory children are typically using static standing as part of their standard care, and the study aims to compare the effects of four months of two types of training regimes, static standing (StS) versus dynamic standing (DyS), on passive range of motion and spasticity in the hips.
Static standing was performed with the use of a standing shell or standing device, while dynamic standing was performed in the Innowalk (Made for Movement).
Material and methods
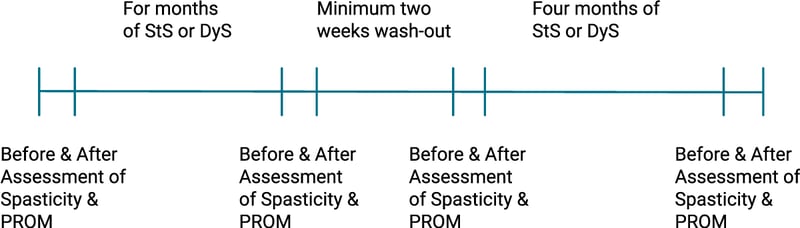
The study was conducted with a cross-over design, including 24 children and 20 children completed the study. Four children did not complete the intervention due to illness, surgery or pain. None of the dropout reasons were related to the exercise intervention. The included children were between 5-17 years of age (mean 11.6 ± 3.6 years), and all children were classified with GMFCS IV (n=11) and V (n=9). All assessments and the interventions were conducted in the children's natural environment (home). Assessments of PROM in the hips (abduction, flexion, extension, Ely’s test, internal andexternal rotation) were performed with a goniometer and spasticity in the hip (flexors, extensors and adductors) was assessed with the use of Modified Ashworth Scale. All assessments were done at baseline, before and after 30 min of StS or DyS, and after four months of intervention, before and after 30 min of StS or DyS (see figure).
Crossover design
- Longitudinal study
- Subjects are randomly assigned to different treatments
- Subjects act as their own controls
- Wash-out period
Results
Passive range of motion in the hip was found to increase after exercise testing of dynamic standing, using the Innowalk for both exercise tests (p< 0.001). Changes in PROM were statistically significantly larger during DyS compared to StS in all movement directions, especially in abduction and external rotation.
When it comes to spasticity measured with the Modified Ashworth Scale, the researchers found that 30 min of StS only reduced the spasticity significantly in hip flexion, while DyS lowered the spasticity in hip flexion, extension and adduction. No changes in spasticity were found for either DyS or StS after four months of exercise training.
Conclusion and implication
The study demonstrated a significant increase in PROM after 30 min and 4 months intervention with dynamic standing in the Innowalk among non-ambulatory children with CP. Spasticity was reduced after 30 min intervention, but no changes were demonstrated after 4 months of intervention.
This new knowledge also indicates that using dynamic standing for intervention in non-ambulatory children with CP does not cause any harm to the children, but rather increases outcomes in relation to passive range of motion and spasticity in the hips compared to typically static standing which is standard care in most countries. The results from the study may help professionals to consider dynamic standing as part of standard care for non-ambulatory children with CP.
If you want more information about the Innowalk and how to get hold on the device for your patients, please contact us for a chat.
Read more:

